About Schistosomiasis
Schistosomiasis, also known as bilharzia or ‘snail fever’, is a parasitic disease carried by freshwater snails that are infected with one of five species from the genus Schistosoma. Schistosomiasis is transmitted by human contact with contaminated fresh water that are inhabited by snails carrying the parasite. Larvae, known as cercariae, emerge from the infected snails and swim in the water until they come into contact with an individual and penetrate the skin. This can occur during a range of normal water contact activities such as collection of drinking water, bathing, washing clothes, swimming or fishing. Once inside the body, the larvae develop into worms which live in the blood vessels for years. Female worms shed eggs which end up in urine and faeces; if infected individuals urinate or defecate into freshwater bodies, the eggs migrate to snails where they hatch and begin the cycle again. The symptoms of schistosomiasis can include frequent painful and bloody urine, abdominal pain and bloody diarrhoea, inflammation and scarring of the bladder, enlargement of the liver or spleen, and where infection persists, bladder cancer may develop. In children it leads to anemia, malnutrition and learning difficulties, thus dramatically impairing their future quality of life and productivity. It is estimated that 258 million people are infected in 78 countries worldwide, though 90% of the infections occur in Africa. Schistosomiasis kills an estimated 280,000 people annually and ranks second only to malaria as the most common parasitic disease.
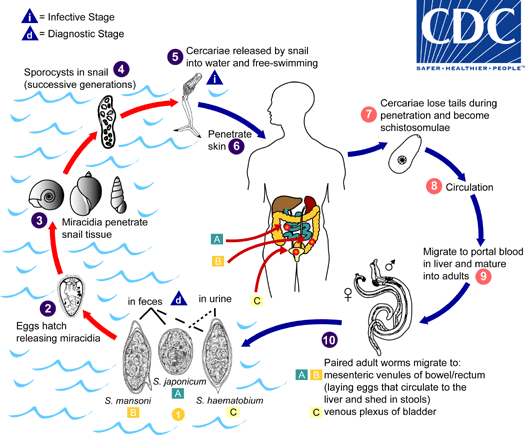
The schistosome life cycles (image adapted from CDC)
About Schistosomiasis Control
Praziquantel is the primary form of treatment, with a single dose of the drug having been shown to reduce the burden of infection and severity of symptoms. However, re-infection will quickly occur when people are re-exposed to contaminated water. Education campaigns about the risks of exposure to contaminated water and improved water supply and sanitation should in theory break the life cycle of the disease. Universal sanitation coverage should prevent the passage of urine and faeces into contaminated water bodies, however there is always a danger of transmission by infected people visiting from elsewhere and urinating or defecating into the water body, or occasional lapses in the usage of sanitation facilities. Mollusciciding has also been suggested as a solution, however there are concerns regarding potential unintended consequences of dosing molluscicides into water bodies and the long-term effectiveness and sustainability of this strategy is questionable, since the snails could return at some point in the future. In some cases there may be alternative water sources (e.g. boreholes) which can be accessed, however often there are no alternative safe water sources available to meet the full water needs of communities in endemic regions. In such cases, therefore, the immediate focus for cutting schistosomiasis transmission must be treating the contaminated freshwater body to provide a safe alternative supply. Our findings from a 2013-14 national mapping programme in Ethiopia relating water and sanitation conditions to schistosomiasis infections supports this logic, since only increased water contact was statistically linked to schistosomiasis infection likelihood, and there was no significant link between schistosomiasis and sanitation.
About WISER
There is currently very limited and incomplete information available regarding the effectiveness of water treatment processes at removing or inactivating cercariae of different Schistosoma. Water treatment solutions for faecal-oral diseases such as cholera may not be effective against cercariae, since they are physiologically completely different from the bacteria which spread such diseases and may have different resistance/sensitivity to treatment. Also, there are no rapid means of detecting cercariae in water samples and determining their viability, which makes assessing the risk and degree of contamination of a water body and testing the effectiveness of water treatment processes as barriers against cercariae very difficult.
WISER (Water Infrastructure for Schistosomiasis-Endemic Regions) is a three-year research programme aiming to address these gaps in critical knowledge through a collaboration between water engineers, synthetic biologists, parasitologists, and social scientists in the UK, Ethiopia and Tanzania, in the hope of developing invaluable new knowledge to guide the design of sustainable water infrastructure for schistosomiasis-endemic regions.
Funding
The WISER project is funded by the UK Government's Global Challenges Research Fund (GCRF) through the Engineering and Physical Sciences Research Council (EPSRC): the grant reference is EP/P028519/1 and further details can be seen here.


Further Reading
Colley DG, Bustinduy AL, Secor WE, King CH. Human schistosomiasis. Lancet. 2014; 383: 2253-64.
Grimes JET, Croll D, Harrison WE, Utzinger J, Freeman MC, Templeton MR. The relationship between water, sanitation and schistosomiasis: a systematic review and meta-analysis. PLoS Negl Trop Dis. 2014; 8: e3296.
Grimes JET, Croll D, Harrison WE, Utzinger J, Freeman MC, Templeton MR. The roles of water, sanitation and hygiene in reducing schistosomiasis: a review. Parasit Vectors. 2015; 8: 156.
Grimes JET, Tadesse G, Mekete K, Wuletaw Y, Gebretsadik A, French MD, et al. School water, sanitation, and hygiene, soil-transmitted helminths, and schistosomes: national mapping in Ethiopia. PLoS Negl Trop Dis. 2016; 10: e0004515.
Kawata K. Slow sand filtration for cercarial control in North Cameroon village water supply. Water Sci Technol. 1982; 14: 491-8.
Kelwick R, Webb AJ, MacDonald JT, Freemont PS. Development of a Bacillus subtilis cell-free transcription-translation system for prototyping regulatory elements. Metab Eng. 2016; 38: 370-81.
Lawson JR, Wilson RA. The survival of the cercariae of Schistosoma mansoni in relation to water temperature and glycogen utilization. Parasitology. 1980; 81: 337-48.
McKerrow JH, Salter J. Invasion of skin by Schistosoma cercariae. Trends Parasitol. 2002; 18: 193-5.
Oliver Gonzalez J, Biaggi N, Rivera Leon J. The effect of chlorine on the motility and infectivity of the cercariae of Schistosoma mansoni. The Puerto Rico Journal of Public Health and Tropical Medicine. 1945; 20: 357-61.
Standen OD, Fuller KA. Ultra-violet irradiation of the cercariae of Schistosoma mansoni. Trans R Soc Trop Med Hyg. 1959; 53: 372-9.
Webb AJ, Kelwick R, Doenhoff MJ, Kylilis N, MacDonald JT, Wen KY, et al. A protease-based biosensor for the detection of schistosome cercariae. Sci Rep. 2016; 6: 24725.